
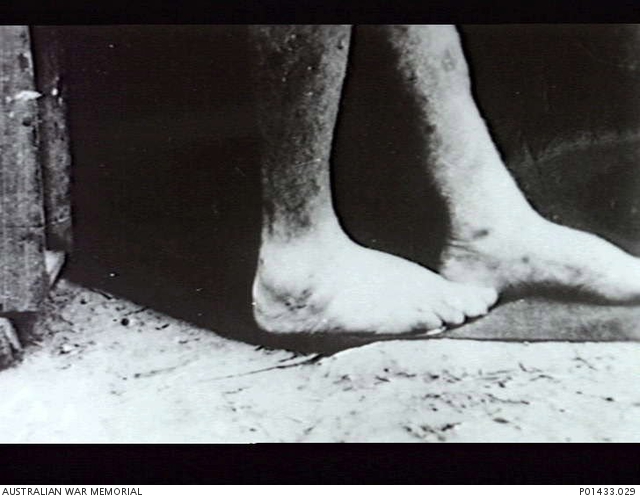
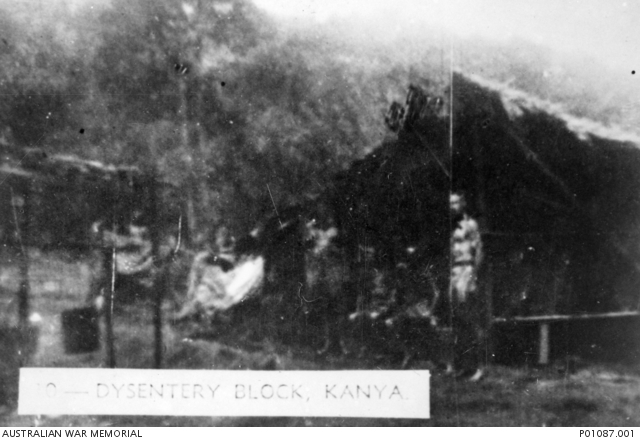
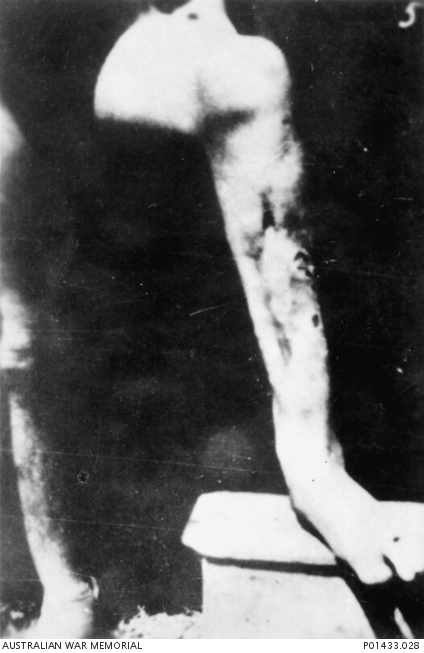
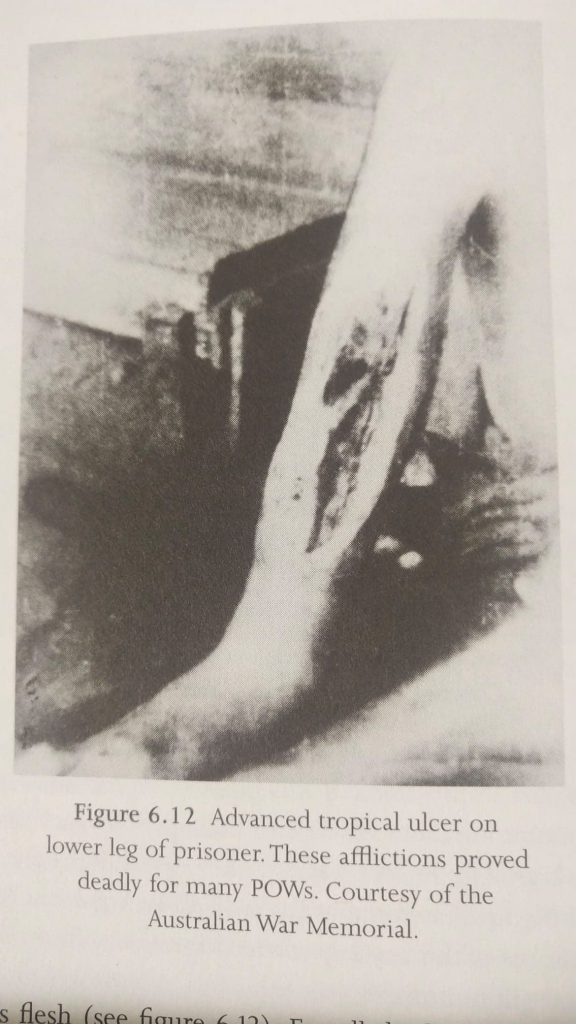
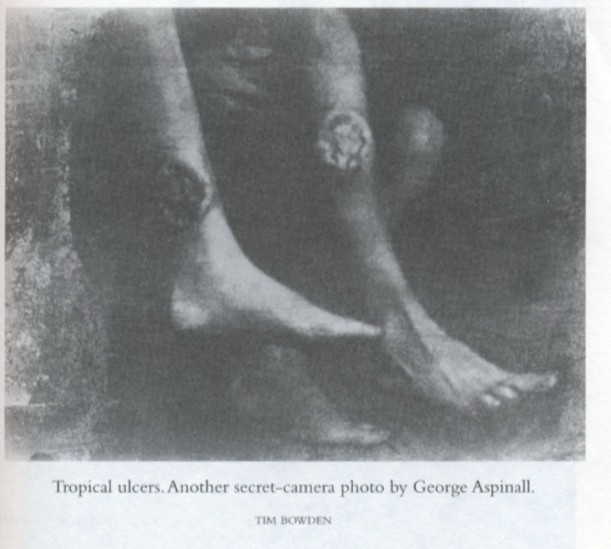
Multiple medical issues compounded the horrific living conditions. Not only were the infectious diseases like malaria and dengue pervasive in many of the areas where the POWs lived and worked, but the lack of adequate food led diseases for lack of proper vitamins. Both their depleted immune systems and lack of medications led to another plaque known as Tropical Ulcer. This comes about when a multitude of bacteria and fungi invade a wound. Small cuts often evolved into large ulcers that severed tendons and exposed bones. These were mostly a problem on the POW’s legs and resulted in many amputations; many POWs did not survive that operation. The lack of adequate sanitation resulted in almost universal bouts of diarrhea and dysentery — either bacterial or amoebic. The latter was so dreaded that the IJA would screen for it prior to transferring POWs to their homeland. Of course, the most dreaded of all was CHOLERA. Some POWs were even inoculated to prevent its spread. Fortunately, the US POWs were spared and none were recorded as dying of cholera although a few were suspected of having a mild cases that they survived. It is also probable that cholera vaccination was part of the normal pre-overseas movement medical regimen of the era. Also, many of the US POWs credit their discipline in drinking only boiled water as preventing the spread of cholera in the camps where they resided.
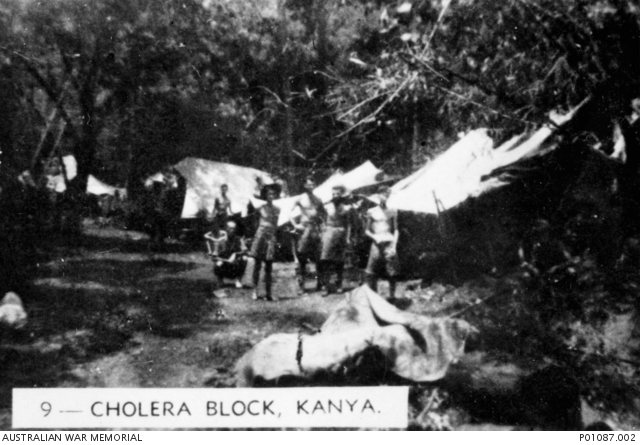
Although it was much less prevalent than the other diseases, cholera was devastating when it struck. It was thought to have originated among the romusha and then spread into the POW camps. These groups often worked side-by-side but were almost always housed separately. The outbreak came at the worst possible time, coinciding with the beginning of the SPEEDO period and the onset of the 1943 monsoon season. Certainly the flow of water as well as the standing water contributed to its spread. While the romusha camps were truly devastated by it the POWs were also heavily hit. The infection seemed to have originated at the Nike area camps Kilo 280) in May and within a few weeks had spread to the Hintok area (Kilo 155). Most likely run-off into the Kwae Noi was the mechanism of spread. But that allowed for some element of dilution as well and the upper camps suffered more. Hardest hit was F Force and then H Force. F Force had been spread over a number of camps in the Thai Highlands and overall 10% of that group was lost to cholera; over 600 men! At Hintok, some 150 cases were recorded with 66 deaths. POW survivor accounts relate horrendous tales of death among the romusha. There is no doubt that the level of discipline and increased efforts at sanitation and boiling drinking water kept the death rates in the POW camps far below those in the neighboring romusha areas. What rudimentary medical interventions the POW medical staffs devised also saved some of the infected men. The romusha had no such assistance. It was these cholera tolls that prompted the IJA to bring medical teams K & L to try to assist them. But with almost no drugs or equipment and the major language barriers, they had little overall success. For the most part, all that was available was to try to identify any new cases early and isolate them from the camp population. Within the smaller H Force over 200 men died.
So great was the IJA staff’s fear of this disease, that they generally avoided any areas where cholera was reported. In a few camps, work on the railway ground to a halt, at least for a few weeks. By this time, some of the US POWs had crossed the border into Thailand at camps that abutted the F Force camps that were affected. There were rumors of a few cases among them that introduced the men to consuming charcoal-like burnt rice as a remedy. A few men stated in later interviews that they believed their physician, CPT Lumpkin, had died of cholera although his official cause of death was listed as dysentery. But then, as quickly as it appeared, the epidemic waned.
As if the nearly 20% death rate among the Allied POWs wasn’t bad enough, diseases were nearly universal – often more than one at the same time. One F Force survivor who worked in the Thai Highlands states that of 1600 men in the camp only 300 were capable of mustering for work on any given day. Malaria and the various forms of dysentery prostrated most men, sometimes simultaneously. Advanced cases of Tropical Ulcers and Beri-beri prevented many from walking. Such men were often made to break rocks for ballast while sitting on stretchers. Even those judged as ‘fit’ were suffering from some malady if only malnutrition.
By Kinvig’s count, F and H Forces suffered the most disease losses: 45 & 27% respectively, Within the British element of F Force the percentage was 61% and the Australians experienced their highest rate of 39%. The single highest count of deaths was at SongKurai with 678 deaths. It is even likely that these figures were ultimately higher, if one were to count the POW-related casualties that occurred soon after liberation.
By comparison, the Tharp Group that worked in Burma (455 men) suffered the greatest losses; a total of 116 deaths (25%) while the overall US POW death rate was 19%.
Medical treatment:
During the construction of the TBR, all resources were devoted to moving the necessary rail way items; no space was available for supplies or medications. What little the various medical personnel had to work with usually came via Khun BoonPong and the V Organization. This changed drastically once the consolidation of the POWs at Kanchanaburi began. Not only did the improved diet there allow many to recover, especially from the vitamin deficiency diseases, but also more medications like Atabrine for malaria were available. Many of the Allied POWs owe their lives to the large hospital camp that was established about that same time in Nakorn Pathom. Reportedly, this new facility was ‘heaven’ for all concerned compared to previous conditions. The physicians had clean ORs and equipment to treat those afflictions that lingered on. Survivors report that many types of operations like appendectomies were able to be performed safely and with great success. One man they could not save, however, was Navy Ensign JOHN STIVER. He was diagnosed with a brain tumor and although he was rapidly evacuated back to the USA, he died in OCT 45 of a glioblastoma.
If there was one bright spot in all of this misery, it was the Nakorn Pathom hospital. An influx of Red Cross medical equipment arrived in APR-MAY 44 and allowed the worst of the POW ill men to be concentrated there along with most of the Allied medical personnel. Drugs and other medical interventions pulled thousands of POWs back from the brink of death. Many ‘routine’ surgical procedures were performed. Rohan Rivett relates that the patient population averaged 5000, with a peak of 8000.
The meaning of words:
Not only did ‘life’ as they knew it change for the POWs (and romusha) but words themselves took on a new meaning, ‘hospital’ for example. Just about every military unit had an assigned doctor and medical staff, but, once in the jungle camps, they had little to offer in terms of medical care. Whatever medical supplies they had at the time of their capture were quickly exhausted. Almost nothing was available by the time they reached the Railway.
It must be remembered that for the Japanese overseers the POW were simply tools. There was no compassion, no concern for their general welfare. They were herded about like cattle and used like tools. To the overseers you were either a worker or not. Those who couldn’t work were useless tools. When a tool breaks you don’t expend much effort to maintain it. When a man was too ill to work, they cut his rations. So a starving man was starved even more.
The POWs worked out ways to surmount these problems. The Japanese paid the POWs a ‘salary’. Somewhere between 10 and 25 cents per day! Most of this money went to supplementing the short-falls in what the IJA supplied.
If only to relieve themselves of the burden, the camp guards generally left the running of the camps to the Allied military officers. Routine chores like cooking, cleaning, collecting fire wood and maintenance of the buildings fell to the POWs. They were allowed a few dozen men to provide these services. Often times it was the ‘light sick’ who were assigned these duties. But if a man was simply too incapacitated to work, he was treated as a broken tool. No need to feed him. As part of this ‘administration’ of camp life, the POWs were often allowed to procure whatever they could to supplement the meager rations the IJA provided. I suspect that this was accomplished largely via the contracts and contacts that Khun BoonPong had. LtCol Dunlop described in great detail how they procured thousands of eggs on a regular basis. These seemed to be plentiful, available and cheap. Most went to feed the sick and recuperating men. This also provided the means for BoonPong to smuggle in other items like medications or simply cash. A few of the POWs commented as to how the camp guards never seemed to care where the POWs got the money to buy these extra items. The POWs referred to these as ‘canteen funds.’ By ‘donating’ his ‘salary’ to these funds, the men knew that if (when) they fell ill, they would be aided by these additional supplies.
As to the ‘hospitals’, the camp medical staff almost always maintained a separate clinic / hospital area. They’d have a daily sick call and tried to keep the sickest men from being assigned to the daily work detail. Many clashes occurred over who was ‘fit’ to work and who was not. But ‘treatment’ for any ailments was more difficult. The small amount of medications that found their way into the camps had to be used with the greatest of care. Triage = deciding who received treatment was difficult for the medical staff. It would benefit no one to use the available drugs to treat a man who was dying of a different ailment. All the POWs seemed to have overlapping illnesses compounding each other. Dysentery and malaria was almost universal. Tropical ulcers were frequent and often debilitating. Of course, general malnutrition and lack of proper vitamins caused much distress as well. The IJA had great difficulty in maintaining their tools!
As the percentage of men in a given camp who were unable to work increased, the IJA would designate a nearby camp as a ‘hospital’ and move the sickest men there. They weren’t being sent for treatment. They were expected to die! They were just being warehoused. Broken tools were collected for disposal! It was purely out of the devotion and dedication of the POW medics that any emerged from those ‘hospitals’.
There were a few exceptions. Once railway work was completed in that area, the ChungKai camp was converted largely to a hospital. Some level of actual treatment was available there. So too, a few hospitals were established in the Kanchanaburi area – two dedicated only to the men in H & F Forces. But these were soon overwhelmed and became ‘death camps’ more than treatment facilities. It wasn’t until the establishment of the large facility at Nakorn Pathom that actual drugs and instruments were made available to treat the many ills that these men brought out of the jungle. Many men owe their lives to the work done at this facility.
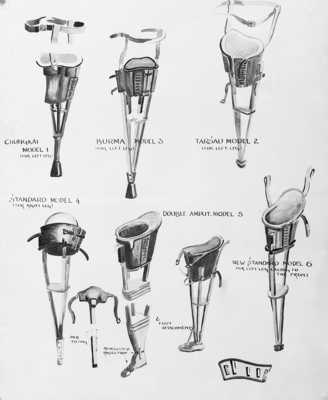
The craftsmen among the POWs worked tirelessly to use whatever they had available to alleviate the suffering of their comrades. They found that bamboo could be used to make almost anything from dental chairs to bedpans. Some camps had a ‘still’ to provide ‘sterile’ water that could be turned into a life-saving infusion with the addition of a pinch of salt.

Surgery was attempted under the most primitive of conditions. It was truly an intervention of last resort. Amputations for Tropical Ulcers were among the most frequent. Appendectomies and other abdominal surgeries were attempted. Many died from sepsis. Anesthesia was rarely available. Somewhat surprisingly, given the nature of the work being performed, injuries were not particularly common. Except that a minor cut or scrape could easily turn into a tropical ulcer. Although he did not seem to have any direct involvement there, in his diary Dr. Dunlop frequently mentioned injuries incurred by the ‘rock drillers’ at Kunyo / HellFire Pass.
The level of callousness and inhumanity demonstrated by the IJA staff is almost beyond belief. In addition to sending the broken tools off to death camps, they rarely expended any effort to treat the maladies that were depleting the work force. They simply called for replacement tools! Hence the arrival of H and F Forces. Little did they know that these new arrivals would soon become the biggest burden to the system. In Section 25, I have tried to relate the horror that developed as these men arrived at their assigned work places just as the monsoon season and cholera struck.
[in Section 31 WHATIFs, I speculate on the concept of a smaller, healthier workforce.]
Not for the faint of heart, below are photos documenting the POW’s medical condition at the time of liberation.














Medical issues are moderately well documented but dental issues plagued many of these men for the rest of their lives. The malnutrition, avitaminosis and ‘grit’ in the rice took a heavy toll of their teeth.