
The short answer to what killed these men is cruelty and neglect.
To the Japanese they were simply tools to be used and discarded. Medically speaking, malaria and dysentery were the main culprits. No adequate or appropriate medications were ever provided. Even the ‘hospitals’ were nothing but a name; they were actually death camps where the sickest men were sent to die.
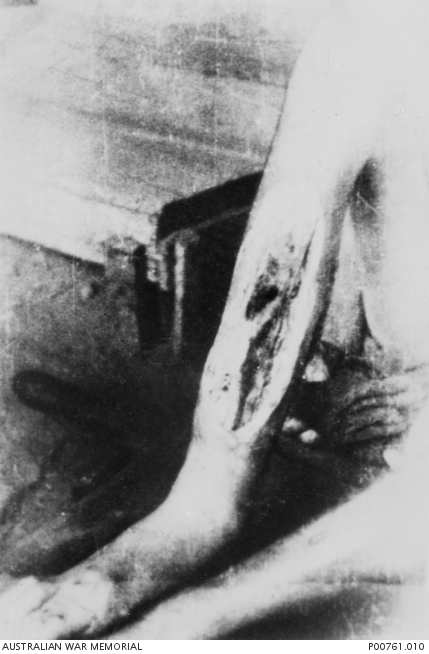
There was even an affliction that was somewhat unique to this situation; it came to be known as Tropical Ulcer[1]. It is not generally found in a Medical Dictionary. It came about when any scratch or cut would become infected with a mixture of bacteria and fungus and perhaps even viruses. These would begin to consume the flesh. The ulcers would enlarge and deepen rapidly until the man was disabled. They most often affected the legs until the man could not walk. Tendons and bones were exposed. The stench was horrible. Early application of a topical antiseptic would likely have prevented most of these. None was available. For many, death would come from gangrene or following amputation of the limb. Amputation was the only true remedy on offer, but few survived that intervention. Other treatments included debriding the wound or introducing maggots that would consume the putrid flesh.


Malaria and dysentery took the life of many but for most they were chronic conditions. Once contracted, they simply lingered. The more common type of malaria was one that recurred every few weeks. The infection would wax and wane. Fever and chills striking every few weeks then relenting again. Never enough to kill just debilitate. Another form, called cerebral malaria, could kill in hours. The mosquitoes that carried it were everywhere; no one was immune. Even the Japanese suffered, although they had access to quinine much of the time.
Dysentery was more than just a chronic diarrhea. It was accompanied by severe abdominal cramping. It too came in different forms. Amebic dysentery could kill rapidly; if caused by bacteria it tended to be a constant companion. Efforts to control its spread were generally futile. It was spread by either direct contact or by the flies that bred in the feces. They were so prevalent that some camps established quotas where each man was required to present with at least 100 flies daily. For some of the hospitalized patients, this became their ‘occupation’.
The most feared disease was cholera. There was a major outbreak in May 43. Fortunately it lasted only a few weeks. It was so feared by the Japanese that they actually provided a crude vaccine to the POWs; none was offered to the Asian workers. Over 1000 POWs are documented as having succumbed. Untold thousands of romusha perished. Most of the POWs had had at least some immunity via vaccine; not so for the romusha. Rapid diagnosis and isolation of cases was reasonably effective in controlling the spread. The camp doctors also insisted that all drinking water be boiled and prohibited swimming or bathing in the river that was thought to be contaminated. It brought work in the affected sections of the TBR almost to a halt.
Between them, dysentery and malaria caused over 50% of the POW deaths. Cholera another 15%. Other infectious diseases: Diphtheria (46), TB (26), Typhus (21), Smallpox (6), Leptospirosis (3) and pneumonia (83) claimed lives. Somewhat more insidious were the various maladies of malnutrition. These developed more slowly but ultimately accounted for about 20% of all deaths. The two forms of Beri-beri (wet and dry) were the most debilitating. About 2% of deaths were deemed to be as a result of ‘natural causes’. The usual afflictions of men, heart attacks, appendicitis, asthma, cancer and the like still claimed lives.
Of course, due to the nature of the work, accidents killed occurred as well. Tropical Ulcers were due mainly to injuries incurred while working or in transit to the work site. Simply walking in the jungle with no shoes or clothes was a hazard. Some men were crushed by falling rocks, others died in falls or drowned. “Friendly fire” from bombing and strafing the trains or bridges, claimed more than a few. Surprisingly few died directly at the hands of their captors. Execution, however, was the penalty inflicted on any who were recaptured in an escape attempt, but more escapees seemed to have perished in the jungles than lived to undergo this penalty.
Cruelty and neglect were, indeed, the underlying causes of all of the 12,000 POW deaths. Once the flow of POWs peaked in April-May 43, the supply system collapsed. It had been barely adequate for the early arriving POWs. As there were more mouths to feed – including tens of thousands of romusha – and the camps were farther from the HQ, that system was incapable of delivering even the most minimal in the way of rations, much less any other necessary supplies. This was all hampered as well by the monsoon rains. The resulting malnutrition exacerbated the other afflictions these men already had. When the ‘tools’ broke, they were simply replaced. No real effort was made to maintain or repair them. More and more ‘hospital camps’ had to be established along the TBR route. At one point, thousands of F Force workers were evacuated into Burma from Thailand to relieve the strain on these camps.
About 70% of all the deaths occurred during the Speedo period of increased work demands as the TBR neared completion (May to October). Nearly 20% more came in the few months following completion as they were consolidated to the ‘rest camps’. It wasn’t until the establishment of the true hospital at Nakorn Pathom in May 44 that many of these afflictions were actually cured. But due to a lack of any interventions what so ever, the romusha continued to die at great rates even in the ‘rest camps’.
[1] The term Tropical Ulcer appears in the medical literature before WW2, but under different circumstances and usually linked to a defined cause. What inflicted these men was different.